Powered By



 Continue with Facebook
Continue with Email
Continue with Facebook
Continue with Email
“Has anyone acquired belly fat from their medications?” asked a member of myHIVteam. “I have belly fat that I’ve fought for years now and I just can’t get rid of it. I’ve tried diets, exercise, and fasting, and I can’t get rid of it. The cocktail I’ve been taking for five or six years has me undetectable with a high CD4 count, but that’s what I think is causing the fat. Any suggestions?”
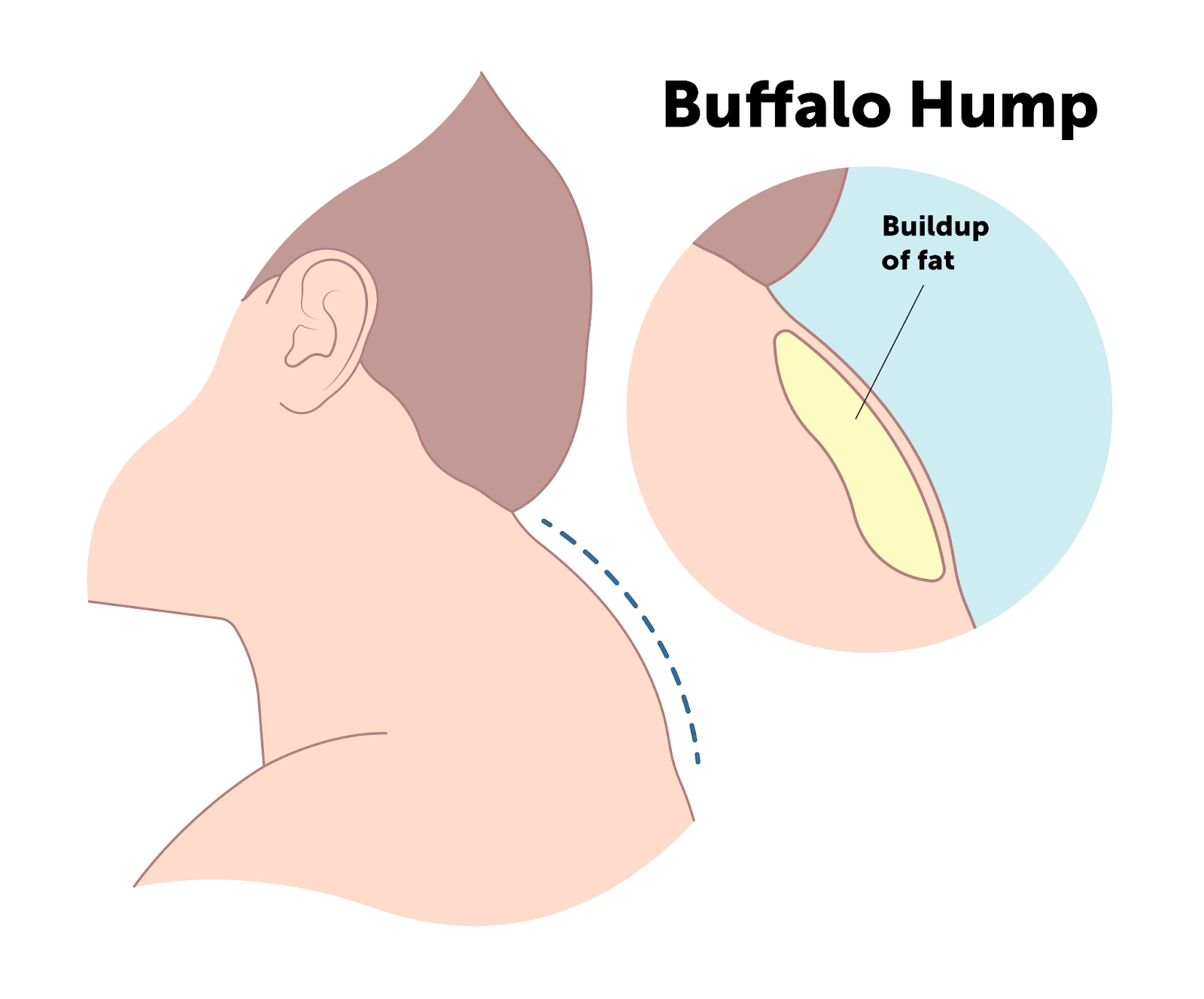
If you or a loved one are living with human immunodeficiency virus (HIV), this myHIVteam member’s story may sound familiar to you. Some people with HIV have lipodystrophy — changes in their body fat. Lipodystrophy may cause a “hard belly” — fat buildup in the abdomen. This is likely a side effect of older HIV medications.
In this article, we’ll discuss what lipodystrophy is, why it develops, and how you can treat it. If you’d like to learn more about why you have lipodystrophy or how to treat it, talk to your doctor.
Throughout your body, you have fat or adipose tissue underneath your skin and around your organs — also called visceral fat. Adipose tissue is more than just fat — it also regulates your hormone levels, stores energy, and keeps you warm.
The term “lipodystrophy” describes changes in how fat is distributed in your body. It encompasses both “lipohypertrophy” — which is fat buildup — and “lipoatrophy” (fat loss). Some people lose fat in one part of the body and have it build up in another. This condition is commonly linked to issues with the body’s metabolism, including unhealthy cholesterol levels and difficulties in how the body uses insulin.
Several forms of lipodystrophy are either inherited through genetics or acquired sometime in a person’s life. Genetic lipodystrophy develops due to gene changes or mutations that cause a person to lose fat tissue.
People living with HIV can develop lipodystrophy if they take certain antiretroviral therapies (ART). They might show signs of losing fat in certain areas, gaining fat in others, or experiencing both at the same time. Specifically, lipodystrophy is associated with taking HIV-1 protease inhibitors as part of an ART regimen. Examples of these medications include:
Cleveland Clinic notes that lipodystrophy is associated with how long a person has been taking ART and how intense their treatment is. The longer a person has taken protease inhibitors, the more likely they are to develop lipodystrophy.
Studies have also found that treatment with nucleoside reverse transcriptase inhibitors (NRTIs) can cause lipodystrophy. You may experience fat loss if you take a regimen that contains a thymidine analog such as zidovudine/azidothymidine (also known as AZT and sold as Retrovir) or stavudine (Zerit).
You may find yourself wondering, “Does HIV cause bloating?” A common symptom of lipodystrophy is an increase in abdominal fat — specifically visceral fat. People with HIV describe this as a “hard belly” because it’s different from softer fat tissue found elsewhere on the body. This symptom can come with unexpected weight gain as well.

Some myHIVteam members have shared what their lipodystrophy looks and feels like. One wrote, “I had lipodystrophy, it began about 15 years ago. All my weight shifted from my arms, legs, face, and chest to my abdomen. I looked atrocious and was very self-conscious.”

Another member shared the following: “I haven’t had a weight problem my whole life, and after a few years on HIV meds, my weight began to blow up. I’m now at 267 pounds after being 180 for most of my adult life. The weird thing is, it isn’t affecting my face, hands, arms, legs, etc. It’s only affecting my mid-section, which is rather bulbous with a sort of ’pregnant look.’”

Changes in your appearance are the primary visible symptom of lipodystrophy. Your adipose tissue plays an important role in controlling hormone levels and metabolic functions. Fat redistribution from lipodystrophy can also lead to high cholesterol levels and diabetes (high blood sugar levels).
Adipocytes are specialized cells in adipose tissue that store fat or lipid droplets. Lipodystrophy stops the body from properly storing fat in adipocytes. As a result, fat begins accumulating in places it’s not supposed to — like the pancreas or liver.
People living with lipodystrophy may develop:
Keep in mind that not everyone with lipodystrophy will develop these conditions.
If you’re looking to get rid of your lipodystrophy, the first step is to talk to your doctor. They can prescribe medications, change your HIV treatment plan, and suggest healthy lifestyle changes to help. Possible treatments for increased fat accumulation include medications such as tesamorelin, surgical interventions, and changes in diet and physical activity.
Tesamorelin (Egrifta) is a medication approved by the U.S. Food and Drug Administration (FDA) for treating lipodystrophy in people with HIV without any active malignancy. It’s a synthetic (lab-made) human growth hormone. Tesamorelin helps your body make more growth hormones to reduce body fat.
Tesamorelin is given as a subcutaneous (under the skin) injection under your belly button. Your doctor will show you how to properly inject the medication.
It’s important to note that tesamorelin isn’t used to help with weight loss — it’s only approved for treating lipodystrophy.
Because most lipodystrophy cases with HIV are caused by medications, your doctor may adjust your treatment plan. The good news is many newer HIV medications are less likely to cause changes in fat distribution.
For example, the NRTIs zidovudine and stavudine are linked to fat loss. Your doctor can switch you to medications containing abacavir (Ziagen) or tenofovir (Viread). Studies show these drugs help redistribute fat tissue and improve your lipid levels.
If you’re unhappy with your appearance due to lipodystrophy, your doctor can refer you to a plastic surgeon. Lipodystrophy can affect your self-confidence, especially if it’s in a cosmetically sensitive area. Plastic surgeons can use implants or tissue transplants to replace missing fat tissue. They can also use liposuction to remove areas of unwanted fat caused by lipodystrophy.
Your doctor may also encourage you to make lifestyle changes with lipodystrophy. Eating a healthy diet and getting regular exercise can help reduce abdominal fat to treat your hard belly. These changes also support your overall health, which is important for boosting your immune system when living with HIV.
Consider adding more of these foods to your diet:
HIV.gov also notes that adults need 150 to 300 minutes of moderate aerobic exercise every week. Examples include walking, running, and biking. It’s also a good idea to add strength training exercises like lifting weights at least twice a week.
If you’ve developed another health condition associated with lipodystrophy, your doctor will treat it as well. It’s important to address high cholesterol and blood sugar levels to avoid more severe complications later on.
Examples of treatments include:
On myHIVteam, people share their experiences with HIV, get advice, and find support from others who understand.
Do you have lipodystrophy from your HIV treatments? Let others know in the comments below.
Get updates directly to your inbox.



Can you have several hiv symptoms at the same time and not have hiv


 Continue with Facebook
Continue with Email
Continue with Facebook
Continue with Email
Continue with Facebook
Continue with Email
Continue with Facebook
Continue with Email
Become a member to get even more



 Join
Join


 Your Privacy Choices
Your Privacy Choices

This is a member-feature!
Sign up for free to view article comments.
All this is Bullshit..doesn't matter about diet.exercise or genetics!!!!..This is Strictly the Medication Side Effects..this happens about 6 years into treatment..it's a nightmare..the only cure is to… read more
We'd love to hear from you! Please share your name and email to post and read comments.
You'll also get the latest articles directly to your inbox.